Healthcare Third-Party Risk Management
Last reviewed: June 2026 | Reading time: 22 minutes | Author: Neotas Intelligence Team
What is healthcare Third-Party Risk Management (TPRM)?
Definition: Healthcare TPRM is the structured process health systems, hospitals, pharmaceutical companies and health technology firms use to identify, assess and continuously monitor risks from external vendors, particularly those who access patient data, support clinical operations or supply regulated products. It covers cybersecurity, HIPAA compliance, FDA obligations, patient safety, financial crime and ESG simultaneously.
Healthcare TPRM is not a cybersecurity discipline with a medical label. It’s a clinical, regulatory and operational function that happens to include cybersecurity. When an EHR vendor fails, hospital revenue cycles collapse. When a pharmacy benefits manager is breached, patients can’t access medication for weeks. When a medical device supplier carries sanctions exposure, the procurement team carries the liability.
Standard TPRM frameworks were designed for financial services. Healthcare requires a different frame: one that accounts for HIPAA’s Business Associate Agreement obligations, FDA supplier qualification requirements, clinical continuity stakes and the patient safety consequences that make a vendor failure in healthcare categorically different from a missed SLA.
According to HIPAA Journal (2026), the average hospital system works with more than 1,000 vendors simultaneously. Every relationship is a potential exposure point for patient data, clinical operations, regulatory compliance and financial stability.
of serious healthcare data breaches involve a third party (HIPAA Journal, 2026)
vendors connected to the average hospital system simultaneously
average cost of a healthcare vendor-related breach (Censinet, 2025)
Americans had PHI exposed in the 2024 Change Healthcare attack
The sector that most resembles healthcare TPRM in complexity is regulated financial services, but even that comparison falls short, because no financial services vendor failure has ever delayed a patient’s chemotherapy.
See also: Complete TPRM guide | Vendor due diligence services | Enhanced due diligence
Key takeaway: Healthcare TPRM spans cybersecurity, HIPAA compliance, FDA obligations, patient safety, financial crime and ESG. It is materially different from TPRM in any other sector because vendor failure has direct clinical consequences, not just financial or reputational ones.
Why healthcare has the highest third-party breach rate of any sector
Healthcare leads all industries in third-party breach rate, average breach cost and regulatory complexity. Three specific factors drive this and understanding them is the starting point for any TPRM programme that will actually work.
Patient safety dependency. A vendor failure in financial services disrupts transactions. A vendor failure in healthcare disrupts care. When Change Healthcare went down in February 2024, pharmacists across the US could not process prescriptions for weeks. That’s not a cybersecurity story. It’s a vendor dependency story with patient safety consequences. No other sector has this dimension.
PHI sensitivity. Protected Health Information sells for an estimated 50 times more on dark web markets than financial data, according to Healthcare IT News (2024). Every vendor touching PHI creates HIPAA liability for the covered entity regardless of where fault lies. The legal obligation for vendor risk management in healthcare is not optional, it’s statutory.
Dual regulatory burden. Healthcare vendors face simultaneous oversight from HIPAA and HITECH (patient data), FDA 21 CFR Parts 820 and 211 (medical devices and pharmaceutical manufacturing), CMS Conditions of Participation (Medicare and Medicaid providers), and an expanding layer of state health data privacy laws. A TPRM programme that satisfies HIPAA may not satisfy FDA supplier qualification requirements. Both must be addressed, and many programmes address neither fully.
Benchmark: 31% of cyber insurance claims in 2024 were linked to third-party vendor issues in healthcare. Breaches involving vendors cost an average of $4.88 million, significantly more than internally-caused breaches. Source: Censinet, 2025.
Most healthcare vendor risk programmes focus their effort on cybersecurity assessment: questionnaires, security ratings, penetration test certificates. What they don’t cover is the non-cyber risk layer: financial distress in a critical supplier before it shows in filings, adverse media about a pharmaceutical manufacturer’s labour violations in a foreign press, beneficial ownership opacity in a medical device distributor, or ESG failures in a clinical staffing agency. These are the risks questionnaire-based programmes structurally can’t detect. They’re also where the highest-value incidents originate.
See also: Healthcare supply chain risk | Financial crime in vendor relationships
Is your vendor programme built for 2026? Most healthcare TPRM programmes are still questionnaire-based and annual. Neotas runs intelligence-led assessments that surface the risks questionnaires structurally can’t find.

What the Change Healthcare breach changed about healthcare TPRM
The February 2024 ransomware attack on Change Healthcare is the defining healthcare third-party risk event of this decade. Understanding what went wrong, specifically is now baseline knowledge for anyone building or auditing a healthcare TPRM programme.
What happened
A ransomware group exploited compromised credentials on a legacy remote access portal that lacked enforced multi-factor authentication. The attack took down prescription processing for pharmacies across the US, disrupted medical claims submissions and payment processing nationwide, and exposed the personal health data of approximately 1 in 3 Americans. Hospitals reported revenue declines of up to 17% in the weeks that followed. Source: Dallas Federal Reserve, 2025.
Why it was a TPRM failure, not just a security failure
Most affected organisations had Business Associate Agreements with Change Healthcare. Many had annual security questionnaires on file. What they didn’t have was a TPRM programme designed to catch the five specific failure modes that created the incident:
- Concentration risk blindness. Change Healthcare processed roughly 40% of US medical claims through a single platform. No individual organisation could eliminate that dependency, but portfolio-level concentration assessment would have revealed the systemic exposure and forced contingency planning.
- Fourth-party dependency gaps. Change Healthcare relied on sub-contractors and cloud infrastructure that created additional exposure points invisible to the covered entities depending on them. HITECH requires Business Associates to impose equivalent safeguards on their own sub-contractors. Most BAAs don’t verify this is actually happening.
- Annual-only monitoring. Multiple security researchers had flagged concerns about Change Healthcare’s security posture in the months before the attack. Continuous adverse media and security posture monitoring would have surfaced this. An annual questionnaire cycle could not.
- No tested outage contingency. Most affected organisations had no tested contingency for claims processing disruption lasting more than 72 hours. This is an operational resilience gap, not a security gap and it should be mapped explicitly by any mature TPRM programme.
- Over-reliance on self-certification. The MFA failure on the legacy remote access portal was a vendor security architecture issue. An independent security architecture review would have identified it. A self-completed questionnaire would not.
“The Change Healthcare event demonstrated that a single third-party failure can generate systemic healthcare disruption at national scale. The lesson is not to improve vendor questionnaires. The lesson is that questionnaire-based programmes are insufficient for critical vendor relationships.”
Dallas Federal Reserve research, 2025 – TPRM and systemic risk in healthcare
What a mature healthcare TPRM programme would have done differently
- Classified Change Healthcare as Critical with continuous monitoring obligations, not annual review
- Required an independent security architecture review, not accepted a self-certified questionnaire
- Mapped concentration risk across the claims processing vendor portfolio with tested contingency plans
- Contractually required MFA enforcement and a documented legacy system decommissioning timeline
- Monitored adverse media and security researcher disclosures in real time, not on a 12-month cycle
See also: TPRM lifecycle: continuous monitoring stage | Concentration risk management
Key takeaway: The Change Healthcare breach exposed five structural failures in healthcare TPRM concentration risk blindness, fourth-party dependency gaps, annual-only monitoring, missing contingency planning, and reliance on self-certified questionnaires. A mature programme addresses all five before a vendor goes critical.
The 7 categories of healthcare vendor and their distinct risk profiles
Healthcare organisations work with a wider range of vendor types than almost any other sector. Each carries a distinct risk profile, regulatory obligation and due diligence requirement. Treating all vendors the same is the most common healthcare TPRM failure – and the most avoidable.
| Vendor type | Risk tier | Primary regulatory obligation | What fails if they fail |
|---|---|---|---|
| EHR / clinical software vendors Epic, Cerner, Meditech and equivalents | Critical | HIPAA BAA, SOC 2, NIST CSF | Mass PHI exposure + clinical operations halt |
| Medical device manufacturers Connected clinical equipment suppliers | Critical | FDA 21 CFR Part 820, ISO 13485, MDS2 | Patient safety event + data breach via connected devices |
| Cloud and SaaS providers Hosting PHI or supporting clinical ops | Critical | HIPAA BAA, SOC 2 Type II, ISO 27001 | Data breach + operational downtime |
| Revenue cycle and billing services Claims processing, billing, coding | High | HIPAA BAA, PCI DSS | Financial fraud + PHI exposure + revenue disruption |
| Diagnostic labs and imaging providers External pathology, radiology | High | HIPAA BAA, CLIA | Clinical error + PHI exposure |
| Telehealth platforms Remote care and virtual consultation | High | HIPAA BAA, FTC Health Breach Notification Rule | Real-time patient data breach + care disruption |
| Clinical staffing agencies Temporary clinical staff with system access | High | HIPAA workforce training verification, background screening | Insider threat + access control failures + PHI breach |
| Pharmaceutical and API suppliers Drug manufacturers, active ingredient suppliers | High | FDA GMP (21 CFR Part 211), ICH Q10, Modern Slavery Act | Drug safety event + ESG violation + supply disruption |
See also: Vendor due diligence services | Vendor due diligence questionnaire guide
Key takeaway: EHR vendors, medical device manufacturers and cloud providers are Critical-tier. Each vendor type carries its own primary regulatory obligation – and a tiering model that doesn’t account for both PHI access and FDA regulatory category will classify vendors incorrectly.
The 6 risk categories every healthcare TPRM programme must cover
A complete healthcare vendor risk programme covers six distinct risk domains. Most programmes cover only the first. The others are where the highest-value incidents originate – and where most competing guides provide almost no useful detail.
Risk Category 1
Ransomware, data breach, unauthorised PHI access, system availability
Every vendor with system access to PHI creates cybersecurity exposure. Assessment criteria for Critical vendors: SOC 2 Type II, ISO 27001, penetration test results (within 12 months), incident response plan, MFA enforcement evidence, data residency documentation. For connected medical devices: MDS2 attestation, software bill of materials (SBOM), patch management procedures, network segmentation evidence.
Risk Category 2
HIPAA, HITECH, FDA, CMS, state health privacy laws
HIPAA violations carry fines up to $1.9 million per violation category per year. (HHS OCR, 2024.) A vendor’s non-compliance event creates direct regulatory exposure for the covered entity even without the entity’s direct involvement. Assessment criteria: regulatory status and licence verification, active HIPAA BAA, documented HIPAA training programme, record of OCR investigations or enforcement actions in any jurisdiction.
Risk Category 3
Clinical operations dependency, device failure, care disruption
This category is what separates healthcare TPRM from every other sector. A failed EHR vendor or medical device supplier is not an IT incident – it is a patient safety event. Assessment criteria: business continuity planning, disaster recovery procedures with tested results, SLA definitions and breach history, clinical dependency mapping, single points of failure identification. Concentration risk assessment is most critical here.
Risk Category 4
Vendor misconduct, regulatory actions, bribery allegations, executive integrity
Standard database checks cannot surface newly emerging adverse media, foreign-language press coverage, or reputational risks that haven’t yet reached structured databases. A pharmaceutical supplier linked to bribery allegations in its home country creates reputational exposure for the health system that procures from it – regardless of whether the health system was aware. Assessment criteria: adverse media screening across traditional, social and emerging sources in 200+ languages, PEP and sanctions screening for vendor executives, beneficial ownership verification, regulatory actions in all jurisdictions.
Risk Category 5
Vendor insolvency, single-vendor dependency, revenue cycle disruption
Change Healthcare demonstrated what happens when a critical function depends on a single vendor with no viable alternative. Assessment criteria: audited financial statements (2-3 years), credit ratings and adverse credit indicators, client concentration analysis (what percentage of the vendor’s revenue does your contract represent?), operational redundancy documentation, concentration risk mapping across the full vendor portfolio. For pharmaceutical procurement: API sourcing concentration by country of manufacture.
Risk Category 6
Labour violations, pharmaceutical supply chain ethics, sanctions exposure
The most underserved risk category in healthcare TPRM. UK healthcare organisations with annual turnover above £36 million have statutory reporting obligations under the Modern Slavery Act 2015. (legislation.gov.uk.) Anti-bribery and corruption (ABAC) obligations in clinical procurement, medical device component sourcing from sanctioned territories, and pharmaceutical manufacturing labour practices all create both regulatory and reputational exposure. Assessment criteria: modern slavery statement review, ABAC policy verification, environmental certifications, labour practice documentation across the supply chain, sanctions screening for supplier-country exposure.
See also: ESG due diligence | Financial crime compliance | Supply chain risk management
Most healthcare TPRM programmes only cover categories 1 and 2. Neotas covers all 6 – including the intelligence layer for adverse media, beneficial ownership and financial distress that questionnaire tools can’t reach.
HIPAA, HITECH and Business Associate Agreement requirements
Direct answer: HIPAA requires covered entities to conduct documented, risk-based due diligence on all Business Associates – any vendor that creates, receives, maintains or transmits Protected Health Information on your behalf. A signed Business Associate Agreement is mandatory before any PHI handling begins. HITECH extended these obligations to sub-contractors, making fourth-party PHI exposure a direct regulatory requirement.
A Business Associate Agreement documents what a vendor is legally obligated to do with PHI. It does not verify the vendor is actually doing it. This distinction is the most consistently misunderstood part of healthcare vendor risk management – and it’s the reason a fully BAA-compliant vendor portfolio can still carry material, undetected risk. A BAA is a legal floor, not a risk management programme.
What a compliant Business Associate Agreement must contain
A BAA is the legal backbone of HIPAA compliance for any vendor relationship involving PHI. Every BAA must address these provisions – missing any one creates a direct HIPAA compliance gap:
- Permitted uses and disclosures of PHI – clearly defined, not open-ended
- Prohibition on unauthorised use or disclosure
- Minimum necessary standard – vendor accesses only the PHI required for the contracted function
- Appropriate safeguards – administrative, physical and technical controls required
- Breach notification timeline – within 60 days of discovery under HIPAA; many organisations contractually require 24-72 hours
- Sub-contractor obligations – the BAA obligation flows to sub-contractors under HITECH; the BAA must require the Business Associate to impose equivalent safeguards on sub-contractors handling PHI
- HHS audit cooperation – vendor must make internal practices available to HHS for compliance review
- Termination and PHI disposition – PHI must be returned or securely destroyed at relationship end; verbal assurance is not compliant
The sub-contractor gap: HITECH extended HIPAA obligations to Business Associates’ sub-contractors. In practice, most BAAs require the Business Associate to impose equivalent safeguards on sub-contractors, but very few covered entities verify this is actually happening. This is the fourth-party risk gap that mature healthcare TPRM programmes must close. Change Healthcare exploited exactly this gap.
| Regulation | Applies to | Core vendor management obligation | Penalty for non-compliance |
|---|---|---|---|
| HIPAA Privacy Rule | All covered entities and BAs | BAA required before any PHI sharing; permitted uses defined | Up to $50,000 per violation, $1.9m annual cap per category |
| HIPAA Security Rule | All covered entities and BAs | Administrative, physical and technical safeguards verified at ePHI vendors | Same as Privacy Rule |
| HIPAA Breach Notification Rule | All covered entities and BAs | BAA must include breach notification; vendor notifies within 60 days | Same as Privacy Rule |
| HITECH Act | BAs and their sub-contractors | HIPAA obligations flow to sub-contractors; strengthened enforcement | Up to $1.9m per violation category per year |
| FDA 21 CFR Part 820 | Medical device manufacturers | Supplier qualification, quality agreements, supplier audits | Warning letters, consent decrees, recalls, prosecution |
| FDA 21 CFR Part 211 | Pharmaceutical manufacturers | GMP compliance, supplier qualification, incoming testing | Warning letters, import alerts, facility shutdowns |
| CMS Conditions of Participation | Medicare/Medicaid providers | Information governance and patient safety requirements influence vendor selection | Loss of Medicare/Medicaid certification |
| Modern Slavery Act 2015 | UK organisations, £36m+ turnover | Annual supply chain transparency statement; active due diligence on labour practices | Reputational consequences; court injunctions |
See also: Full TPRM regulatory requirements | TPRM policy guide
Key takeaway: A compliant BAA must cover permitted PHI uses, safeguards, breach notification timelines, sub-contractor obligations and HHS cooperation rights. HITECH makes fourth-party PHI exposure a regulatory requirement – not just good practice. The largest HIPAA fine in 2024 was $950,000 for inadequate vendor oversight.

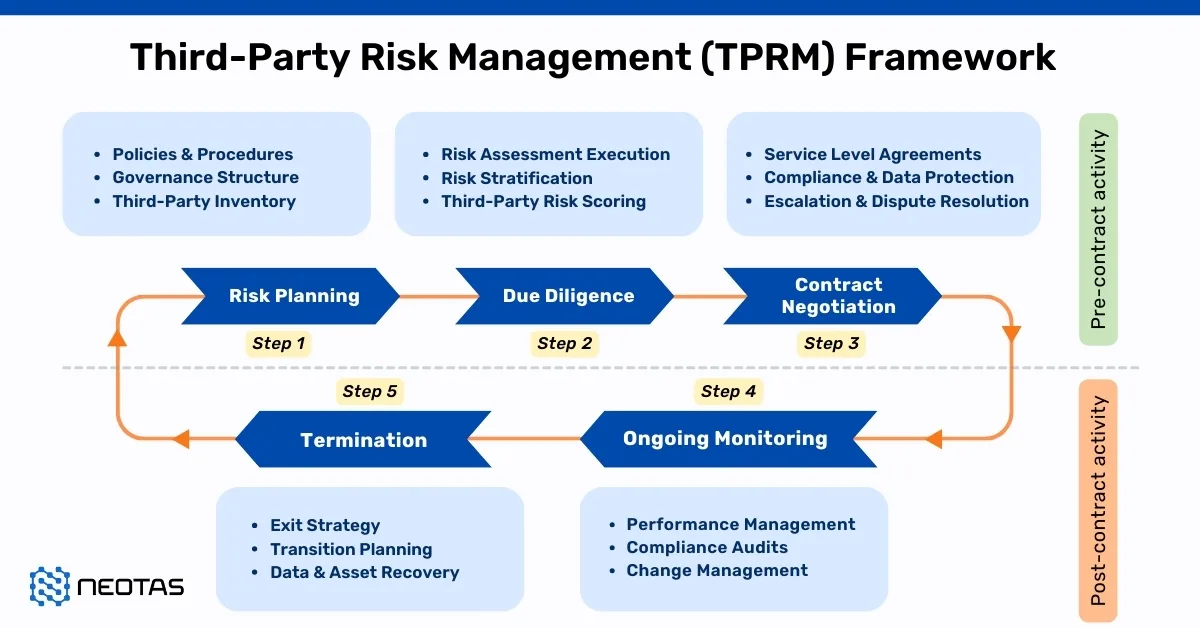
The healthcare vendor risk assessment process: 7 stages
Healthcare vendor risk management runs a continuous lifecycle, it does not end at onboarding. Most healthcare TPRM failures happen not because the stages are unknown, but because specific stages are skipped, compressed or handed to technology without clear ownership. For full methodology: TPRM lifecycle guide.
| Stage | What happens | Healthcare-specific requirement | Most common failure |
|---|---|---|---|
| 1. Vendor inventory | Map every vendor with PHI access, clinical system access or patient-critical supply role | Include all Business Associates and HITECH sub-contractors handling PHI | Most hospitals find 30-50% more vendors than their records show |
| 2. Risk tiering | Classify by PHI access, clinical criticality, regulatory category, concentration risk | BAA requirement determines minimum due diligence threshold; clinical criticality determines tier | Classifying by vendor category rather than actual PHI function and access level |
| 3. Pre-onboarding due diligence | Tier-proportionate assessment before any PHI access begins | Critical vendors: intelligence-led full assessment. Standard: questionnaire + BAA verification | Relying entirely on self-completed questionnaires — can’t detect what vendors won’t disclose |
| 4. BAA and contract controls | Signed BAA before any PHI handling; contract provisions for breach notification, audit rights, sub-contractor disclosure | BAA must satisfy all HIPAA required provisions; sub-contractor obligations must flow through | Generic BAA templates missing HITECH sub-contractor obligations or breach timelines shorter than 60 days |
| 5. Ongoing monitoring | Continuous monitoring for adverse media, regulatory actions, security incidents, financial distress | Annual questionnaire alone does not satisfy HIPAA’s “ongoing” due diligence requirement | Annual-only reviews — most incidents happen between review cycles, not during them |
| 6. Issue management | Defined escalation paths and documented response when monitoring flags a risk | HHS OCR examines issue management records during investigations | Alerts fire but no defined action path exists — monitoring without response is not compliance |
| 7. Offboarding | PHI return or certified destruction, access revocation, BAA termination, documented closeout | HIPAA requires documented PHI disposition at relationship end | Residual PHI access left active months after a relationship ends |
See also: Full TPRM lifecycle guide | TPRM questionnaire limitations | Enhanced due diligence for healthcare vendors
Stage 3 and Stage 5 are where most healthcare TPRM programmes break down. Neotas runs intelligence-led pre-onboarding assessments and continuous monitoring for Critical and Important-tier healthcare vendors. No questionnaire required from the vendor.
The intelligence gap: what healthcare vendor questionnaires structurally cannot find
Every guide in this space recommends vendor questionnaires. None of them acknowledges the fundamental limitation: a questionnaire only surfaces information the vendor is willing and able to disclose. It cannot detect what vendors don’t know about themselves — and it cannot detect what vendors are unwilling to share.
In healthcare, the risks that questionnaires miss are precisely the ones most likely to cause serious incidents.
What questionnaire-only programmes miss in healthcare
- Adverse media in non-English press. A pharmaceutical manufacturer with documented GMP violations in its home country press. A medical device distributor linked to bribery allegations in an emerging market. A clinical staffing agency with labour practice violations in regional publications. Structured databases capture this weeks or months after the fact, if at all.
- Beneficial ownership opacity. A healthcare SaaS vendor owned through multiple holding companies, one layer of which contains a party connected to a sanctioned individual. No questionnaire asks about the full beneficial ownership chain. OSINT investigation surfaces it.
- Financial distress signals. A pharmacy benefits manager in early financial difficulty that has not yet appeared in public filings. Adverse credit indicators, supplier payment delays, executive departures and debt covenant breaches are visible through financial intelligence monitoring months before formal disclosure.
- Regulatory actions in other jurisdictions. A medical device manufacturer with an active FDA 483 observation in one product line that did not appear in their questionnaire response because it was considered resolved.
- Sub-contractor concentration risk. Two critical EHR vendors both using the same cloud infrastructure provider in the same region. Neither vendor discloses this because it’s proprietary. Network analysis surfaces the shared single-point-of-failure.
- Executive-level integrity risks. A vendor’s senior leadership team with undisclosed connections to public officials in procurement jurisdictions — a direct FCPA or UK Bribery Act risk for the health system if undetected.
Multiple security researchers raised concerns about Change Healthcare’s security architecture in the months before the February 2024 attack. This information was available in open-source forums and security researcher publications. An annual questionnaire cycle would not have captured it. Continuous monitoring that scans adverse media, security researcher disclosures and regulatory flags would have. This is what intelligence-led healthcare TPRM is specifically designed to do.
Neotas addresses this gap through OSINT-enhanced vendor screening — combining adverse media monitoring across 200+ languages, beneficial ownership analysis, financial intelligence, sanctions proximity screening and social media monitoring into a single assessment workflow. For healthcare organisations, this is most critical for Tier 1 vendors: EHR providers, medical device manufacturers, pharmaceutical supply chain partners and revenue cycle operators. See enhanced due diligence services and OSINT tools in vendor screening.
Key takeaway: Healthcare vendor questionnaires cannot detect adverse media in foreign press, beneficial ownership opacity, emerging financial distress, cross-jurisdiction regulatory actions, sub-contractor concentration risk or executive integrity issues. These are the gaps that intelligence-led OSINT screening closes.
FDA requirements and medical device supplier risk management
Medical device suppliers and pharmaceutical manufacturers operate under a separate regulatory framework from HIPAA-governed vendors. FDA oversight creates specific TPRM obligations that most general vendor risk frameworks don’t address — and that most healthcare TPRM guides don’t adequately cover.
FDA 21 CFR Part 820 — medical device supplier qualification
FDA’s Quality System Regulation requires medical device manufacturers to implement documented supplier qualification and oversight processes. This means: supplier evaluation criteria, approved supplier lists, incoming inspection procedures, periodic supplier audits and quality agreements defining each supplier’s responsibilities. For health systems procuring medical devices, the vendor’s FDA compliance status is itself a TPRM due diligence item — a device manufacturer operating under an FDA consent decree or with active 483 observations creates downstream risk for the healthcare organisation using their products.
ISO 13485:2016 — medical device quality management
ISO 13485 is the international standard for medical device quality management systems. Certification requires documented supplier evaluation, risk-based purchasing controls and ongoing supplier performance monitoring. Certification is a minimum quality threshold for procurement — it does not substitute for active intelligence-led due diligence on regulatory standing and reputational profile.
MDS2 attestation and software bills of materials
Connected medical devices create simultaneous clinical and cyber risk. Two assessment documents apply specifically:
- MDS2 (Manufacturer Disclosure Statement for Medical Device Security): A standardised form disclosing cybersecurity capabilities, data handling practices and network connectivity. Requiring a current MDS2 from all connected device vendors is a healthcare-specific due diligence step that general TPRM frameworks don’t include.
- Software Bill of Materials (SBOM): FDA’s 2023 medical device cybersecurity guidance requires manufacturers to provide an SBOM — a complete inventory of software components in the device. This lets health systems assess whether any component contains known vulnerabilities or relies on software from sanctioned entities.
Pharmaceutical supply chain risk
Pharmaceutical procurement creates a distinct risk profile. Active Pharmaceutical Ingredient sourcing concentration — where a generic drug’s API comes from a single manufacturing region — creates both supply disruption risk and geopolitical sanctions risk that standard vendor questionnaires don’t assess. The FDA’s drug shortage data shows that concentration in API manufacturing creates systemic vulnerability for the US pharmaceutical supply chain. (FDA Drug Shortages database.)
For UK pharmaceutical organisations, the Modern Slavery Act 2015 requires annual supply chain transparency statements covering due diligence on labour practices across the supply chain — including API manufacturers and contract research organisations. This is an ESG obligation that sits inside the TPRM framework.
See also: Supply chain risk management | ESG due diligence for pharmaceutical supply chains
Key takeaway: Medical device suppliers require FDA 21 CFR Part 820 and ISO 13485 assessment in addition to standard vendor risk checks. Connected devices require MDS2 attestation and SBOM review. Pharmaceutical supply chains require API sourcing assessment and, for UK organisations, Modern Slavery Act compliance verification.
FDA compliance status is a vendor risk indicator most TPRM programmes don’t check. Neotas includes FDA enforcement action screening — 483 observations, consent decrees, warning letters — as part of every medical device and pharmaceutical vendor assessment.
How to build a healthcare TPRM programme: 8-step guide
Building a healthcare TPRM programme that satisfies HIPAA, FDA and clinical continuity requirements simultaneously requires a specific order of operations. Most programmes fail by jumping to technology before the governance model exists. For a full roadmap: TPRM framework guide.
- Define scope, ownership and governance. Assign programme ownership — typically a joint function between CISO, Chief Compliance Officer and General Counsel in healthcare. Define what “vendor” means for your organisation (include Business Associates, sub-contractors, staffing agencies, clinical equipment suppliers). Get board-level sign-off on the programme charter before anything else happens.
- Build the vendor inventory. Use procurement records, accounts payable data, IT system access logs and clinical department interviews. Include all Business Associates and HITECH sub-contractors. Expect to find 30-50% more vendor relationships than current records show.
- Design the healthcare-specific risk tiering model. Tiering criteria for healthcare must include: PHI access level, BAA requirement (yes/no), clinical criticality (what fails if this vendor fails?), FDA regulatory category, concentration risk and jurisdictional exposure. Minimum three tiers: Critical, Important, Standard. No vendor handling PHI should sit below Important.
- Design due diligence processes by tier. Critical (Tier 1): full intelligence-led assessment across all 6 risk categories. Important (Tier 2): structured questionnaire plus independent adverse media and financial screening. Standard (Tier 3): questionnaire plus BAA verification.
- Build BAA and contract standards. Develop a compliant BAA template covering all HIPAA and HITECH required provisions. Establish minimum contractual provisions for non-BAA vendors: audit rights, breach notification timelines, sub-contractor disclosure, exit assistance and PHI disposition.
- Implement continuous monitoring for Tier 1 and 2 vendors. Annual questionnaires alone don’t satisfy HIPAA’s ongoing due diligence requirement. Automate adverse media alerts, sanctions list changes and financial health signals for all Critical vendors. Monitoring frequency: Critical vendors monthly or real-time; Standard vendors annually.
- Define issue management and escalation paths. Document who receives monitoring alerts, what action is required at each escalation level, and what triggers board notification — before the first alert fires. HHS OCR investigations examine issue management records closely.
- Establish governance reporting. Board-level reporting on TPRM programme status, key risk indicators and open issues. Maintain a vendor register in a format accessible for OCR audits. Formally document the programme in a TPRM policy. See TPRM policy template.
See also: TPRM framework guide | TPRM policy guide | TPRM maturity model
5 common healthcare TPRM mistakes (from real programme reviews)
These are the five failures that appear most consistently when reviewing healthcare vendor risk programmes — not theoretical gaps, but patterns from actual programme assessments.
1. Treating the BAA as the due diligence
A signed BAA documents obligations. It does not verify the vendor is meeting them. Many healthcare organisations check the BAA box and consider vendor risk managed. These are two separate activities.
2. Vendor count surprises
Programmes built on procurement records alone consistently miss 30-50% of actual vendor relationships. IT-shadow vendors, department-level SaaS tools and staffing agencies with system access are the most common blind spots.
3. Annual reviews as “ongoing” monitoring
HIPAA requires ongoing due diligence. HHS OCR does not define this as annual. For Critical vendors, annual questionnaires are point-in-time snapshots with 12-month gaps between them, not ongoing monitoring.
4. Questionnaire-only Critical vendor assessment
Self-certified questionnaires can’t detect adverse media in foreign press, financial distress signals before formal disclosure, or beneficial ownership opacity. For Tier 1 vendors, this is the most common gap between perceived and actual risk coverage.
5. No tested contingency for Critical vendor failure
Most healthcare TPRM programmes identify Critical vendor dependencies but don’t have tested alternatives or continuity procedures if those vendors fail. Change Healthcare turned this from a theoretical gap into a documented incident costing hospitals an average of 17% revenue.
How Neotas supports healthcare TPRM
Neotas is an intelligence-led third-party risk management provider, rated in the Chartis FCC50 as a leading financial crime compliance technology provider. Healthcare organisations use Neotas specifically for the intelligence layer that questionnaire platforms and cybersecurity rating tools can’t provide.
| Capability | Healthcare risk category | What it delivers |
|---|---|---|
| Intelligence-led vendor due diligence | All 6 risk categories | OSINT-enhanced assessment across cybersecurity posture, financial health, regulatory standing, adverse media, beneficial ownership and ESG indicators |
| Adverse media screening | Reputational and adverse media risk | 200+ languages, traditional press, social media and emerging sources |
| Beneficial ownership analysis | Financial crime and reputational risk | Multi-layer corporate structure investigation for sanctions exposure, PEP connections and undisclosed conflicts |
| Financial distress monitoring | Financial stability and concentration risk | Early warning from payment behaviour, credit indicators, executive departures and regulatory filings |
| ESG and supply chain screening | ESG, Modern Slavery and ethical risk | Pharmaceutical API sourcing assessment, labour practice screening, ABAC indicators, UK Modern Slavery Act evidence |
| Continuous monitoring | All categories — ongoing | Automated alerts for adverse media, sanctions changes, regulatory actions and financial health signals |
| Financial crime compliance integration | Regulatory and financial crime risk | AML, KYC and sanctions screening embedded in vendor due diligence |
Healthcare TPRM in practice: what intelligence-led screening found
Each engagement below involved a vendor that looked clean on standard database checks. Intelligence-led screening found the risk before it became the client’s problem.
Supply chain risk identified before contract signature
A healthcare procurement team needed supply chain due diligence beyond standard database checks on a prospective pharmaceutical partner. OSINT screening surfaced adverse media, undisclosed regulatory actions and reputational risk indicators invisible to structured data sources. The engagement prevented a high-value partnership with a materially compromised supplier. Read the supply chain OSINT case study
ESG screening uncovers vendor supply chain exposure
A global organisation commissioned ESG risk screening on its vendor population. Labour practice violations and environmental breaches were identified in a Tier 2 supplier — the kind of sub-contractor visibility that TPRM programmes must demonstrate under Modern Slavery Act and CSDDD obligations. Read the ESG supply chain case study
Third-party risk found through OSINT screening
A regulated organisation needed vendor due diligence beyond questionnaire-based assessment. Neotas OSINT screening surfaced adverse media, undisclosed corporate connections and reputational red flags that structured data sources had missed entirely. Read the TPRM OSINT case study
Network analysis uncovers beneficial ownership risk
Standard corporate checks on a procurement counterparty returned clean results. Neotas network analysis mapped undisclosed corporate relationships that created material risk exposure — precisely the beneficial ownership opacity issue that affects pharmaceutical and medical device supply chain due diligence. Read the network analysis case study
Further reading
The foundational guide — lifecycle stages, regulatory requirements across DORA, FCA and OCC, risk categories, maturity model and best practices.
OSINT-enhanced vendor assessment covering financial health, adverse media, regulatory standing and beneficial ownership.
Fourth-party and Nth-tier supply chain risk — pharmaceutical API sourcing concentration, medical device component risk and sub-contractor mapping.
How intelligence-led EDD works — OSINT screening, adverse media analysis, beneficial ownership investigation and financial crime indicator screening.
Step-by-step framework build — risk tiering methodology, due diligence design by tier, governance structure and board reporting.
What a compliant TPRM policy must cover — contract standards, BAA provisions, monitoring frequency and documentation obligations.
Modern Slavery Act compliance, ABAC obligations, pharmaceutical labour practice assessment and medical device component sourcing verification.
AML, KYC and sanctions screening in healthcare vendor relationships — pharmaceutical supply chains and medical device distributors with complex ownership structures.
Detailed methodology for each of the 7 lifecycle stages — vendor inventory through offboarding, with common failure points at each stage.
Frequently asked questions: healthcare third-party risk management
What is healthcare TPRM?
Healthcare TPRM (Third-Party Risk Management) is the structured process health systems, hospitals, pharmaceutical companies and health technology firms use to identify, assess and continuously monitor the risks created by external vendors, suppliers and service providers. It covers cybersecurity, HIPAA compliance, FDA supplier qualification, patient safety, financial crime and ESG risk simultaneously. Unlike TPRM in other sectors, healthcare TPRM carries direct patient safety stakes and dual regulatory oversight from both HHS and FDA. A vendor failure in healthcare isn’t a missed SLA — it can delay medication dispensing or take diagnostic equipment offline.
What is a Business Associate Agreement (BAA)?
A Business Associate Agreement is a legally binding contract required under HIPAA between a covered entity and any vendor (Business Associate) that creates, receives, maintains or transmits Protected Health Information on the covered entity’s behalf. It must define permitted PHI uses, require appropriate safeguards, set breach notification timelines, include sub-contractor obligations under HITECH, and specify PHI return or destruction at termination. A BAA documents legal obligations — it does not verify the vendor is actually meeting them. That verification is a separate, ongoing due diligence requirement.
What are the HIPAA requirements for a Business Associate Agreement?
A compliant BAA must define permitted uses and disclosures of PHI, prohibit unauthorised use, apply the minimum necessary standard, require administrative, physical and technical safeguards, set a breach notification timeline within 60 days of discovery, flow sub-contractor obligations through under HITECH, specify HHS audit cooperation rights, and require PHI return or certified destruction at relationship end. HHS OCR fines for inadequate vendor oversight reach up to $1.9 million per violation category per year. HHS OCR enforcement
Is a BAA enough to manage healthcare vendor risk?
No. A BAA is the legal minimum, not a risk management programme. It documents what a vendor is contractually obligated to do with PHI but does not verify the vendor’s actual security posture, financial stability, beneficial ownership structure or regulatory standing. Organisations that treat the signed BAA as the completed due diligence step are the most common source of undetected vendor risk in healthcare. A BAA should be paired with risk-tiered due diligence and ongoing monitoring, not treated as a substitute for them.
What does health TPRM stand for?
Health TPRM stands for Healthcare Third-Party Risk Management. It refers to the application of TPRM disciplines to the specific risk profile of healthcare organisations — covering the HIPAA Business Associate framework, FDA supplier qualification requirements, clinical continuity obligations and the patient safety stakes that distinguish healthcare vendor risk from all other sectors. “Health TPRM” and “healthcare TPRM” are interchangeable and mean the same thing.
Why is healthcare the highest-risk sector for third-party breaches?
Healthcare has the highest third-party breach rate of any sector due to patient safety dependency (vendor failure directly affects clinical outcomes), PHI sensitivity (patient data is estimated at 50 times the dark web value of financial data), and regulatory complexity (simultaneous HIPAA, HITECH, FDA, CMS and state-level obligations). The average hospital works with over 1,000 vendors simultaneously. Healthcare breaches involving vendors cost an average of $4.88 million — significantly more than internally-caused breaches. Source: HIPAA Journal, 2026.
What happened in the Change Healthcare breach and what does it mean for healthcare TPRM?
In February 2024, a ransomware group exploited compromised credentials on a legacy remote access portal without enforced MFA at Change Healthcare, the US’s largest pharmacy claims clearinghouse. The attack disrupted prescription processing and medical claims nationwide for weeks, exposed data on approximately 1 in 3 Americans, and caused hospital revenue declines of up to 17%. The TPRM lesson: most affected organisations had BAAs in place and annual questionnaires on file. What they lacked was continuous monitoring, concentration risk assessment, tested contingency planning and independent security architecture review. Source: Dallas Federal Reserve, 2025.
How does healthcare TPRM differ from general vendor risk management?
General vendor risk management focuses on cybersecurity, operational performance and commercial risk. Healthcare TPRM adds: HIPAA and HITECH regulatory obligations with defined penalties, mandatory Business Associate Agreements for PHI-handling vendors, FDA supplier qualification requirements for medical devices and pharmaceutical suppliers, patient safety as a direct stake, and ESG and Modern Slavery obligations for clinical supply chains. The dual regulatory overlay and patient safety stakes make healthcare TPRM materially more complex — and the consequences of failure are clinical, not just financial.
How do you tier healthcare vendors by risk level?
Healthcare vendor risk tiering uses five criteria: (1) PHI access — does this vendor create, receive, maintain or transmit PHI? (2) BAA requirement — is this vendor a Business Associate under HIPAA? (3) Clinical criticality — what fails if this vendor fails, and does it affect patient care directly? (4) FDA regulatory category — is this a medical device manufacturer or pharmaceutical supplier with FDA obligations? (5) Concentration risk — what percentage of a critical function does this vendor represent? Critical vendors (Tier 1) require full intelligence-led assessment across all 6 risk categories. No PHI-handling vendor should be below Tier 2.
What does a healthcare vendor risk assessment include?
A complete Tier 1 healthcare vendor risk assessment includes: cybersecurity assessment (SOC 2 Type II, ISO 27001, penetration test results dated within 12 months), HIPAA compliance verification (BAA status, documented safeguards, breach history), financial health review (audited financials, credit indicators, client concentration), adverse media screening across traditional press, social media and 200+ language sources, beneficial ownership verification, FDA compliance status for device and pharma vendors, business continuity and disaster recovery with tested results, and sub-contractor disclosure. Tier 3 vendors use a structured questionnaire with BAA verification only. See enhanced due diligence services.
What is continuous monitoring in healthcare vendor risk management?
Continuous monitoring in healthcare TPRM is ongoing surveillance of active vendor relationships beyond the initial assessment. It covers: adverse media alerts for vendor misconduct or regulatory actions, sanctions and PEP list changes affecting vendor ownership, financial health signals indicating vendor distress, regulatory enforcement actions in any jurisdiction, cybersecurity incident notifications, and changes to vendor sub-contractor relationships. For Critical vendors, continuous monitoring replaces annual-only review cycles. Annual questionnaires alone do not satisfy HIPAA’s “ongoing” due diligence requirement — HHS OCR does not define ongoing as once per year.
What are the FDA requirements for medical device supplier risk management?
FDA 21 CFR Part 820 requires medical device manufacturers to implement documented supplier qualification: supplier evaluation criteria, approved supplier lists, incoming inspection, periodic audits and quality agreements. ISO 13485:2016 certification is the international equivalent and a minimum due diligence threshold for procurement. Connected medical devices require MDS2 attestation (cybersecurity disclosure form) and, per FDA’s 2023 guidance, a Software Bill of Materials (SBOM) listing all software components in the device. Active FDA 483 observations or consent decrees on a supplier are critical risk flags that should trigger immediate escalation. FDA.gov
What is fourth-party risk in healthcare?
Fourth-party risk in healthcare is the exposure that flows through your direct vendors (third parties) to their own sub-contractors, cloud providers and technology partners. HITECH explicitly requires Business Associate obligations to flow to sub-contractors — making fourth-party PHI exposure a direct HIPAA compliance issue, not just a cybersecurity concern. The Change Healthcare breach exposed this gap: affected health systems had BAAs with Change Healthcare but no visibility into Change Healthcare’s own infrastructure sub-contractors. A mature healthcare TPRM programme maps fourth-party dependencies for all Critical vendors. See supply chain risk management.
What are the penalties for HIPAA vendor compliance failures?
HIPAA violation penalties range from $100 to $50,000 per violation, with an annual cap of $1.9 million per violation category. Penalties are tiered by culpability: lack of knowledge ($100-$50,000), reasonable cause ($1,000-$50,000), wilful neglect corrected ($10,000-$50,000), wilful neglect not corrected ($50,000, $1.9m annual cap). Criminal penalties apply for intentional PHI misuse, up to 10 years imprisonment. The largest HIPAA fine in 2024 was $950,000 against a healthcare provider specifically for inadequate Business Associate oversight. Inadequate vendor due diligence is itself an enforcement trigger, not just the breach that follows. HHS OCR enforcement history
How does intelligence-led screening differ from questionnaire-based healthcare TPRM?
Questionnaire-based healthcare TPRM relies entirely on self-reported vendor information. It cannot detect: adverse media in non-English press, emerging financial distress before formal disclosure, beneficial ownership opacity in multi-layer corporate structures, regulatory actions in other jurisdictions, sub-contractor concentration risk or executive-level integrity issues. Intelligence-led screening uses OSINT to independently verify and investigate vendor risk across all these dimensions, surfacing risks the vendor cannot or won’t disclose. See Neotas enhanced due diligence.
What is healthcare SaaS vendor risk?
Healthcare SaaS vendor risk covers cybersecurity, data privacy and operational risks from cloud-based software providers that health systems rely on for clinical, administrative or revenue cycle functions. SaaS vendors handling PHI are Business Associates under HIPAA, requiring signed BAAs and documented safeguard verification. Key assessment criteria: SOC 2 Type II certification, data residency and geographic controls, multi-tenancy data isolation, breach history, sub-processor disclosure (a HITECH fourth-party obligation) and business continuity capabilities. The proliferation of SaaS in healthcare has significantly expanded the Business Associate landscape compliance teams must manage.
What is healthcare supply chain risk management?
Healthcare supply chain risk management covers risks across the full chain of suppliers that deliver clinical products, pharmaceutical ingredients, medical devices and support services to health systems. It extends beyond direct vendors to API manufacturers, component suppliers, logistics partners and contract research organisations. Key risks include pharmaceutical supply disruption from API concentration in a single manufacturing country, medical device component sourcing from sanctioned territories, labour practice violations (Modern Slavery Act obligations), and fourth-party cybersecurity exposure from vendor sub-contractors. See Neotas supply chain risk management.
What is a healthcare vendor risk management framework?
A healthcare vendor risk management framework is the structured set of policies, processes, controls and governance mechanisms an organisation uses to manage third-party vendor risk consistently within its healthcare regulatory context. It defines how vendors are inventoried, tiered, assessed, contracted, monitored and offboarded within the constraints of HIPAA, HITECH, FDA and applicable state health privacy laws. A healthcare-specific framework incorporates Business Associate identification, BAA mandatory provisions, risk tiering criteria that include clinical criticality and FDA regulatory category, and monitoring protocols that satisfy HIPAA’s ongoing due diligence requirement. See Neotas TPRM framework guide.
How does concentration risk apply to healthcare vendor risk management?
Concentration risk in healthcare TPRM is the exposure created when a critical clinical or operational function depends on a single vendor or a small group of vendors with no tested alternative. Change Healthcare’s roughly 40% share of US medical claims processing is the defining example: no individual organisation could eliminate the dependency, but the systemic exposure was visible and the contingency plan was absent. Concentration risk assessment maps which critical functions have single-vendor dependency, what percentage of each vendor’s revenue your contract represents, and whether contingency procedures have been tested. For pharmaceutical API sourcing, concentration by country of manufacture is the equivalent risk dimension. See supply chain concentration risk management.
Build a healthcare TPRM programme that goes beyond questionnaires
Neotas works with compliance leads, procurement directors and risk teams at health systems, pharmaceutical companies and health tech firms across the UK and US. We cover the intelligence layer that questionnaire-only programmes can’t reach.
Chartis FCC50 recognised. Used across healthcare, life sciences, insurance and financial services.
No commitment required. We confirm availability within 1 working day.